|
|
|
|
|
| Basic Wire-Handling Strategies for Chronic Total Occlusions | 3/10
|
Carefully evaluating the lesion enables the physician to choose the optimal treatment modality and gain insight into potential problems before even starting the procedure. It is an essential part of strategy design. Even those doctors with plenty of experience with normal lesions, should realize the considerable difference in interpreting usual lesions and CTOs. Great care has to be paid to things that do not come up with usual lesions.
i) Occlusion Duration: It is often difficult to measure exactly how long a vessel has been occluded, but even in the absence of a detailed history of myocardial infarction, you can get a good idea of the occlusion duration by obtaining a detailed medical history from the patient. Some CTOs presenting with bridging collaterals, which appear quite old, turn out to be relatively young. Be careful, in these lesions a stiff wire may easily and suddenly push through the occlusion and create a false lumen. Since occlusion duration has an important impact on wire selection and handlingtechnique, finding out as much as you can about the patient’s history is a great advantage.
ii) Lesions Proximal to the CTO and Vessel Shape: As I have outlined above, the location of the coronary artery ostium, the bifurcation direction and the shape of the vessel all have an impact on choice of guide catheter, but when there is a lesion at the entry to the CTO or proximal to it, the guide catheter can cause ischemia or coronary artery dissection. All available coronary angiographic information must be carefully analyzed when choosing the correct guide catheter and identifying the best way to maneuver it. This is especially important in the RCA, as I have already said, and though it will depend on the individual circumstances, one may want to pre-dilate ostial or proximal lesions, and implant a stent. This often results in improved wire handling and can also reduce and prevent complications.
When there is tortuosity or bending of the vessel proximal to the CTO, this will have an effect not just on what wire one chooses and how it is handled, but will also be an important factor in the positioning of the balloon catheter. Thinking of ways to improve wire maneuverability before one begins a procedure, can not only reduce procedure time and cut down on the amount of contrast medium use, but it can reduce unnecessary wire handling and limit injury to the vessel.
|
||||||||||||||||||
|
|
||||||||||||||||||
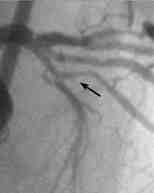
| Figure 2: Patient with Chronic
Total Occlusion in proximal LAD This CTO is located immediately after the bifurcation of the diagonal, and though it is unclear how long it has been occluded, the patient’s medical history suggests that it may be a number of years. CAG does not clearly identify the CTO ostium, (white arrows show an area that looks like the entry but black arrows show an actual dimple). It is only by the AP cranial view that the dimple be seen at all, and that only when viewed by frame by frame slow motion. This could easily be missed under normal CAG. |
||||||||||||||||||
iii) CTO Morphology: Lesion morphology, (i.e. whether or not there is a dimple) affects success rate, and care must be taken not to overlook dimples when looking at the coronary angiogram. It is important to look at the images from a number of angles and frame by frame (Figure 2), while at the same time, looking to see if there are any potential recanalization channels or existing lumina inside the CTO. Pursuing paths through the CTO along these channels doesn’t guarantee that one won’t create a false lumen, but they can often suggest a way through for the wire. It often happens that if one can accurately guide the wire through one of these channels, it makes it easier to get through to the distal true lumen. If the CTO is old and bridging collaterals have formed, however, it is necessary to differentiate between the recanalization channels and any lumina with dilated vasa vasorum connected to the bridging collaterals. This is not an easy task, and if the wrong channel is chosen, there is risk of causing a perforation.
Bends in the vessel inside the CTO
are also sometimes missed. These are especially difficult to anticipate accurately
in long CTOs in the RCA and LCX. The only real way to get a feel of what path
a vessel is going to take is to have as much experience as possible. During
coronary angiography, one should instinctively bear in mind the bends at proximal
and distal segment of RCA, as well as at proximal segment of LCX.The same is
true for middle segment of LAD. Even when these segments have not been imaged
clearly, one should always know what to expect at these segments. Also, calcification
configuration can often be a good indicator of vessel shape, so it can sometimes
be useful to delay infusion of the contrast medium for 2-3 heart beats during
fluoroscopy or coronary angiography, to get a better image of the calcification.
Another tip is that when the proximal and distal portions of the occlusion seem
to slip out of alignment with each heartbeat; this is a sign of tortuosity inside
the CTO.
|
|||||||||||||||||||||||||||||||||||||||
|
|
|||||||||||||||||||||||||||||||||||||||
| Figure 3: Morphlogy of distal
end of CTO affect wire passage In tapering CTOs like the one shown, the only possible point for the wire to penetrate is at (a), and if you miss this point even by a little, such as (b) or (c), it’s not only very easy to create a false lumen, but almost impossible to try again to make a second penetration point at (a). |
|||||||||||||||||||||||||||||||||||||||
|
|||||||||||||||||||||||||||||||||||||||
|
|
|||||||||||||||||||||||||||||||||||||||
| Figure 4: CTO with tight
distal bend When the distal portion of the CTO is located on a tight bend, if you try to go straight for the main trunk, as in (b), you risk creating a false lumen as in (c) and (d). If, the side-branch is co-axial to the wire, going instead for the side-branch, as in (e), will give you a much better chance of getting through the distal fibrous cap at the end of the CTO. |
|||||||||||||||||||||||||||||||||||||||
As important it is to look closely at morphology in the proximal part of the CTO, it is equally important to see what the situation is at the distal end. For this, it is crucial to make sure to get a good image of the distal vasculature supplied by collateral flow. This is also important in gauging lesion length. One can sometimes mistake a short CTO for a long one. and set the penetration point too far distal, and thus make a false lumen. When the distal end of the CTO is wider than the proximal part, there is a high probability that the lesion will be hard, and the distal fibrous cap thick and hard, unless oneu knows from the medical history that the CTO is relatively recent. When there is a tapering distal portion and a chronic build up of jagged hard plaque around the true lumen, one can expect it to be extremely hard to get the wire through. There is only a single correct penetration point at the distal end of the CTO because once one makes a false lumen anywhere in the vicinity of the fibrous cap, the true lumen becomes very difficult to locate (Figure 3). So, for this reason, when the wire is near the distal end of the CTO, it is vital that the wire is steered such as not to miss the distal cap and create a false lumen. This means that identifying the shape of the end of the occlusion is a valuable source of information for determining how to maneuver the wire. It is hard to tell by coronary angiography, but one will find that if the plaque at the distal end of the CTO is soft, the opposite will happen and the wire will cross quite easily. In summary,, it is important to pay attention to lesion morphology at the distal end of the occlusion as well as to any bends in the vessel. If there is a major bend in the vessel, making sure to find the true lumen is crucial (Figure 4).
|
|
|
|
|