|
|
|
|
|
| Basic Wire-Handling Strategies for Chronic Total Occlusions | 4/10
|
iv) Collateral Flow: Monitoring collateral flow when maneuvering the wire is also a very important part of the strategy. The older the CTO, the more influence age has on initial success. It is relatively straightforward to identify the channels supplying and receiving collateral blood flow, as well as the main collateral channels (sometimes because there are more than one of these, one must identify all the main channels as they are competing for blood flow), there are pitfalls. For instance, if one of the supply channels is an atrial branch or conus artery branch bifurcating from an proximal RCA, the catheter tip can find itself i down one of these branches and collateral flow will not show up on the angiogram. If one is aware of this possibility it can be prevented.If one makes a point of checking to see that collateral flow is reaching as far as the cap of the distal end of the CTO, he sometimes notices collateral flow that is not showing up on coronary angiography, because of competition for blood flow or a negative jet. In LAD CTOs a separat Conus branch may be thesupply channel for collateral flow. In these cases, the distal cap of the CTO will be visualized from the Conus, and the image of the LAD trunk will be receiving collateral flow from the posterior descending artery via the septal branch, or the right ventricular branch. It is not uncommon to miss, on coronary angiography, collateral flow coming from the separate Conus branch Collateral flow from the Conus, though, is extremely important in cases like this to assist wire handling.
When the CTO is in the RCA, it is important to check that collateral flow is being supplied to the posterior descending artery andposterolateral branch, and when the CTO is in the LCX, whether it is coming from the peripheral left posterolateral branch or the atrial circumflex branch. These can be important sources of information, if you cannot obtain good distal images when maneuvering a wire, or for preventing ischemia.
There is also the possibility that during the procedure, the tip of the guide catheter will reduce collateral flow. Be especially careful that the tip doesn’t block the collateral supply channel in the proximal portion of the ostial RCA.
Looking at collaterals is a useful and valuable way of gauging the distal true lumen. Knowing whether the vessel bifurcates towards the distal end of the CTO, knowing the angle of bifurcation, whether there is stenosis or plaque at the bifurcation ostium are - as I will show later in the section on Side Branch Technique - extremely important. As I have already said, finding out whether there is diffuse distal plaque build up is also a vital part of pre-procedural strategy-formulation.
c) Contra-lateral Injection: Using contra-lateral injection is an indispensable part of CTO strategy. It is no exaggeration to say that most expertise as to how to maneuver the CTO wire comes from the use of this technique. It does not just tell one how to move the wire forward, but continually provides information during the procedure and while the wire is moving into the distal course of the true lumen and any bifurcations. One really cannot tackle CTOs without contralateral injection, and all operators should understand that using it gives you the best possible map of the vasculature.
There are still a number of points to be careful of when using contralateral injection:
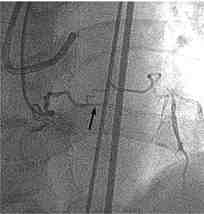
i) The guide catheter and coronary angiography catheter may interfere with each other. This happens quite frequently, and may be very difficult or impossible to engage the guide catheter. Using the left radial artery approach for the coronary angiography catheter is one way to solve this. One should avoid using AL shapes for both the guide catheter and the coronary angiography catheter. If there is a problem getting the coronary angiography catheter stable in position, it may be easier to use either a soft 5Fr guide catheter + Transit® + guidewire, or a 4Fr or 5Fr coronary angiography catheter + wire combination (Figure 5)
Figure 5
Figure 5: Case with guide wire used to stabilize catheter for CAG of conus branch.
When selectively attempting CAG of the conus branch, fixing the catheter position and avoiding wedging can be tricky, but a good way round this is to insert a guide wire through the catheter.ii) ischemia may be a problem. When one does contralateral injection in the RCA, he must be careful that the catheter does not find its way deeper into the vessel and cause ischemia. If the coronary angiography catheter keeps getting wedged in the conus artery branch, passing a guidewire along the coronary angiography catheter and forcing it back is a good way of preventing freeing it from the wedge.
iii) the amount of contrast medium may be prohibitive. One tends to use a large volumes of contrast medium during contralateral injections, but this depends on how it is done. I find that “super-selective” angiography (usually with the Transit®) is a good way to keep down the amount of contrast medium that is used. Alternatively, routine use of 4F catheters for contralateral injection will help limit the amount of contrast.
It may be obvious that it is a good idea to do coronary angiography from as many directions as possible before beginning the procedure, but it is also imperative that one assess the relation of the guidewire tip to the distal cap of the CTO from a number of angles, both during fluoroscopy and coronary angiography. Some operators do work from only one angle, but their success rates suffer as a result. Even experienced operators should remember that they can get carried away during a procedure and forget to look at the vessel from multiple directions. Be careful.
It goes without saying that the best imaging view to monitor the relative positions of the distal cap of the CTO should be taken, but even though in order to get a 3D image of the relative positions, it can sometimes be useful to move an intensifier during injection. Similarly, a biplane device is a good way to cut down on contrast volume, but one should not limit himself to just two angles.
|
|
|
|
|