
|
|
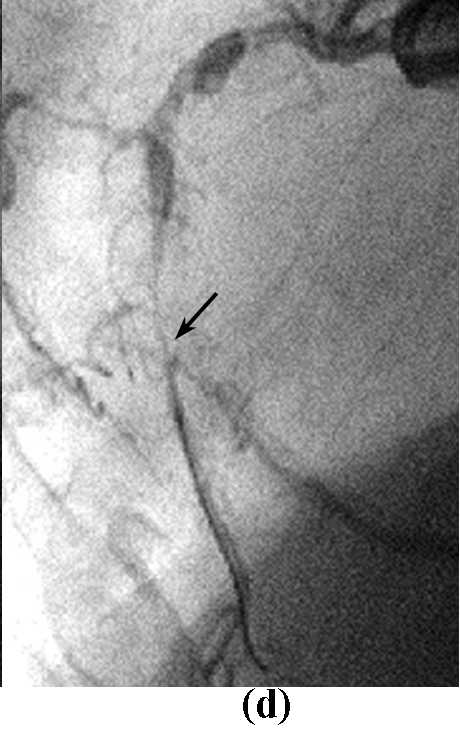
Figure 16: Breaking through the distal fibrous cap using the side wire technique
In this patient, the wire is restricted by heavy calcification throughout the
RCA and by a sharp proximal bend. In addition to this, another bend in the distal
portion of the CTO and diffuse plaque build-up meant I had to attempt to make
my perforation by turning the wire towards the AM diagonal and trying to get
at the distal fibrous cap from the AM ostium (a)(b). The problem was that the
wire had gone slightly too far down into the AM diagonal (c). I therefore had
to change to a rota-wire (d), and rotablate with a 1.25mm burr. I managed to
position the burr in the ostium correctly and not too far, and avoid any distal
vessel perforation (e). After rotablation, with the plaque at the AM branch
excised (f), the wire advanced easily into the main trunk (g).